Opioids and the Crisis of the White Working Class
A sense of betrayal seems to lie just behind today’s political discourse—a feeling of being left behind, a suspicion that those at the top, in media, corporations, politics, academia, and finance, have motives and goals at odds with those of the broader population. Put simply, Americans of all backgrounds fear and loathe a hostile elite. Political memes like “the Deep State,” “the 1%,” “Drain the Swamp,” “the Davos Set,” and “Masters of the Universe” each capture this feeling of alienation, suspicion, and helplessness.
Historically speaking, class rivalry is hardly unusual. But a political situation in which a ruling elite is actively hostile towards the population it governs is quite rare, but not without precedent.
With conservatives, the immigration question brings these feelings of betrayal to the surface, perhaps in their most pronounced form. The popularity of the chant “Build The Wall!” reveals this. “The Wall” is tacitly understood, by those who resonate with it, as a means of re-gaining control over their communities and country. In turn, both liberals and those who could properly described as political and social elites view “The Wall” as far more than a barrier to illegal entry: it is an attack on their values, if not a direct attack on them.
More than any other issue, the immigration question represents a yawning gap between elite and popular opinion, between the Republican establishment and its White voting base. If U.S. immigration policy since 1965—beginning with the Hart-Celler Act of that year—had ever been presented honestly, as leading directly to minority status for Whites by the mid-21st century, and if White people could vote on this basis while they were still some 85-90 percent of the country, it might never have passed. In a very real sense, this policy is illegitimate and we should view its effect in changing the demographic balance of the country as illegitimate. As I have argued based on the historical evidence, U.S. immigration policy stemming from the 1965 sea change is the result of the activism of an ascendant Jewish elite that now holds a dominant position in our culture—dominant in the sense that they are able to severely punish those who dissent from this project of racial replacement by, for example, slanting media coverage and threatening loss of job, and it is able to significantly reward those who go along with it—everyone who has any aspirations to public life understands what can and cannot be said, and great careers await those who go along with the system.[1] This change in the demographic balance of the country was accomplished by promulgating a new “science” of race, stemming ultimately from Franz Boas and his protégés and entrenched in the top academic institutions, by founding and funding lobbying groups and positive media coverage.
The second component of this onslaught is that so many Whites are enthusiastically engaged in this project. They understand the reward-punishment choices and go along with them. Furthermore, many Whites are genuinely motivated by feelings of guilt and a desire to be virtuous—a virtue defined by incessant propaganda emanating from elite universities and media and facilitated by a science of race and by invidious, politically and ethnically motivated historical accounts of the history of White America. Others are motivated by misguided, suicidal dedication to “principles”—especially the individualist inheritance of Constitutional government, individual liberty, etc.
The theme here is the same—betrayal by a hostile elite and complicity of many of our own people targeting a vulnerable population which they hold in contempt.
Recently, the phenomenon of “The White Death” has entered the public consciousness and received comment by mainstream and elite sources.[2] In a nutshell, working class Whites are dying at an increasing rate, whereas most studies show the mortality rates of non-Whites decreasing. For working-class Whites, almost every indicator of social dysfunction and depression are increasing: they are committing suicide; they are using drugs more often and with damaging results; they failing to establish families; they are sleeping more, watching television and streaming services, etc.
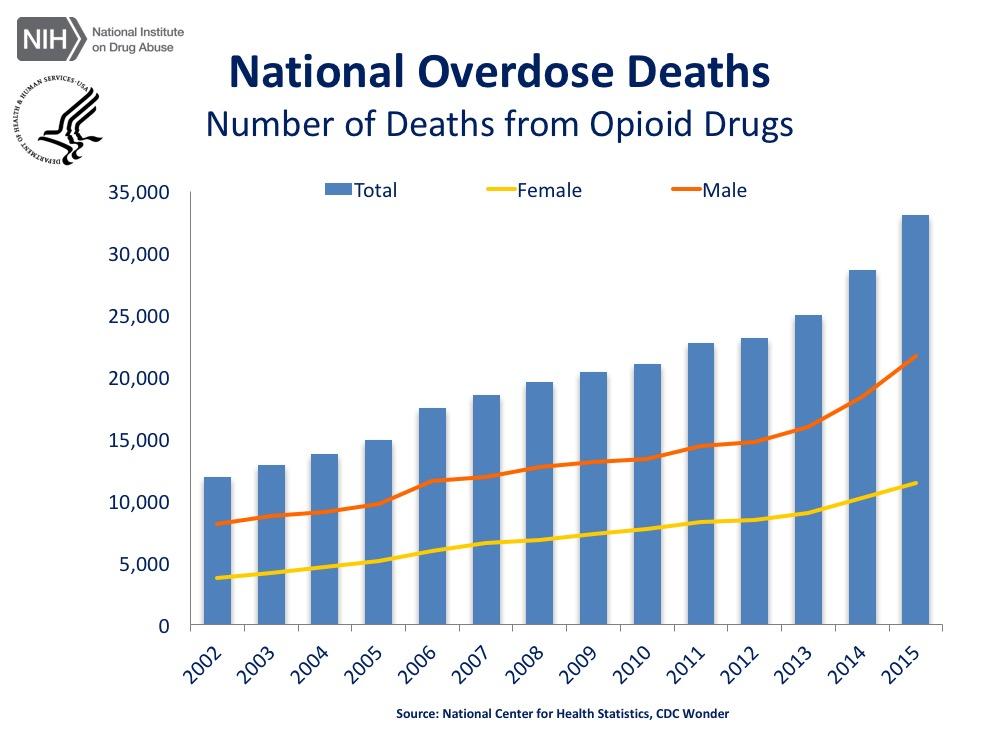
The opioid crisis is an intense expression of this broader phenomenon. The past two decades have witnessed a major increase in the use of prescription opioids as a means of pain management. Abuse has become rampant and a black-market economy has arisen. The most common of these drugs is oxycodone (marketed under the names OxyContin and Percocet); the synthesized drug fentanyl, which resembles heroin and morphine in its potency,
As the New York Times reports,
The current opioid epidemic is the deadliest drug crisis in American history. Overdoses, fueled by opioids, are the leading cause of death for Americans under 50 years old — killing roughly 64,000 people last year, more than guns or car accidents, and doing so at a pace faster than the H.I.V. epidemic did at its peak.[3]
Fatalities resemble those of a World War. Some 250,000 people, mainly Whites, have died as a result of the abuse. The journal STAT has estimated that some 500,000 might die as a result over the next decade.[4]
This story of the opioid epidemic cannot be properly told without an understanding of the dynamic between the working class and the American and global elite. This dynamic is similar in many ways to the framework of my book The Culture of Critique, except that, rather than positions at prestigious universities, contracts with top-notch publishers, and media influence, it’s mainly about the financial benefits to the Sackler family resulting in the deaths of around 250000 mainly White people—and still increasing year over year. As in The Culture of Critique, this was a top-down movement based ultimately on fake science created at the highest levels of the academic medical establishment, motivated by payoffs to a whole host of people ranging from the highest levels of the academic-medical establishment down to sales reps and general practitioner physicians.
A lot of the discussion centers around research by economists Anne Case and her husband, Nobel-winning Angus Deaton claiming that the increase in mortality comes from “deaths of despair [that] come from a long-standing process of cumulative disadvantage for those with less than a college degree. The story is rooted in the labor market, but involves many aspects of life, including health in childhood, marriage, child rearing, and religion.”[5]
My basic theory here is that it’s not really about despair. I argue there are two things at work here: one is the decline in our culture generally brought about by the 1960s’ counter-cultural revolution affecting health in childhood, marriage, child rearing, and religion. But added to that is a very specific situation involving opioid drugs that in turn is linked to academic researchers willing to falsify data for financial gain, a corrupt pharmaceutical industry, especially Purdue Pharma owned by the Sackler family, and lax government regulation of drugs because of manipulation by the pharmaceutical industry.
The General Cultural Decline in the West since the 1960s
First the general decline in our culture. One of the themes of The Culture of Critique is that in general people on the lower end of the bell curve have been disproportionately affected by the cultural changes that have come to the fore since the 1960s. This was especially a theme of the chapter on psychoanalysis that focused on the effects of the sexual revolution. In general people on the lower end of the bell curve benefit more from strong social supports — in particular, support for marriage and against out-of-wedlock births. In my previous life teaching developmental psychology, the chapter on the family had charts showing that beginning in the 1960s there have been dramatic increases in out-of-wedlock births and divorce, resulting in many more children being raised without fathers. This opened up new fields in child psychology as psychologists investigated the effects on children of these cultural shifts. The results are clear: divorce, single parenting, and births out of wedlock are strong risk factors in a wide range of child problems, including delinquency, criminality, poor performance in school, poor physical and emotional health and early mortality—exactly the outcomes emphasized by Case and Deaton.
A theme of The Culture of Critique is that Jews were fundamental to the success of the countercultural revolution of the 1960s, whether it was as leaders of campus radicals or promoting the sexual revolution. Chapter 4 is dedicated to the assault on traditional Western sexual culture by psychoanalysis and related movements, and I emphasize that this revolution had a disparate impact on different IQ groups. Jews suffer to a lesser extent than non-Jews from the erosion of cultural supports for high-investment parenting and the decline in religious belief. Because Jews are a relatively high-IQ group, they have been relatively immune from these negative effects.
A major theme of The Bell Curve is that divorce and other measures of family dysfunction are more common at the lower end of the IQ distribution. The only reason I use IQ is that it is studied much more and can be very precisely measured, but you could get the same findings by using impulse control. People at the lower end of the IQ distribution also have more difficulty controlling their impulses, they are more prone to instant gratification rather than long-term planning and would be expected to be more prone to drug addiction.[6] As a result, they suffer more from the erosion of cultural supports for high-investment parenting—delaying sexual intercourse, not getting pregnant before marriage, etc. When I was going to high school no one was having sex in my school—a Catholic school where the traditional supports were strongly in place. But we have to understand that since the 1960s there has been a very successful attack on this culture.
There’s no question that traditional religious belief was a major part of those cultural supports. Quoting from Chapter 4 of The Culture of Critique:
As [Norman] Podhoretz (1995, 30) notes, “it is in fact the case that Jewish intellectuals, Jewish organizations like the American Jewish Congress, and Jewish-dominated organizations such as the ACLU… have ridiculed Christian religious beliefs, attempted to undermine the public strength of Christianity, and have led the fight for unrestricted pornography.” The fact is that psychoanalysis as a Jewish-dominated intellectual movement is a central component of this war on [non-Jewish] cultural supports for high-investment parenting. …
Although other factors are undoubtedly involved, it is remarkable that the increasing trend toward low-investment parenting in the United States largely coincides with the triumph of the psychoanalytic and radical critiques of American culture represented by the political and cultural success of the counter-cultural movement of the 1960s.
We should never forget that this war was inaugurated by Sigmund Freud, a fake scientist who hated the people and culture of the West and imagined himself as Hannibal conquering Rome. And of course, people like Freud have come a long way in accomplishing just that. This was not a revolution motivated by love of humanity but by hatred toward the people and the culture of the West.
These trends have occurred in all races but they affect Blacks more than Whites because on average Blacks are lower on impulse control and around one standard deviation lower than Whites on IQ. Blacks have always had higher percentages of out-of-wedlock births, but the gap widened to the point that now ~72% of Black births are out-of-wedlock compared to ~36% for Whites, with Asians having even lower rates (~17%).[7] This fits with Phil Rushton’s ranking of evolved race differences.. Sexual behaviors are heritable (genetically influenced): a study showed that before the sexual revolution, age of first intercourse was not influenced genetically because there were strong social norms against pre-marital sex; if there is no variation, then there can be no genetically influenced variation by definition, and as a result age of first sexual intercourse was not heritable.[8] So in my high school, since no one was having sex, age of first intercourse was not heritable. But after the sexual revolution it became heritable: people prone to a slow life history pattern and high control of impulses were more able to delay onset of sexual behavior, avoid childbirth outside of marriage, and stay married. As would be expected given Rushton’s theory, the sexual/cultural revolution has been disastrous most of all for Blacks. In 1965, 24 percent of Black infants and 3.1 percent of White infants were born to single mothers compared to ~72% and ~36% now.[9]
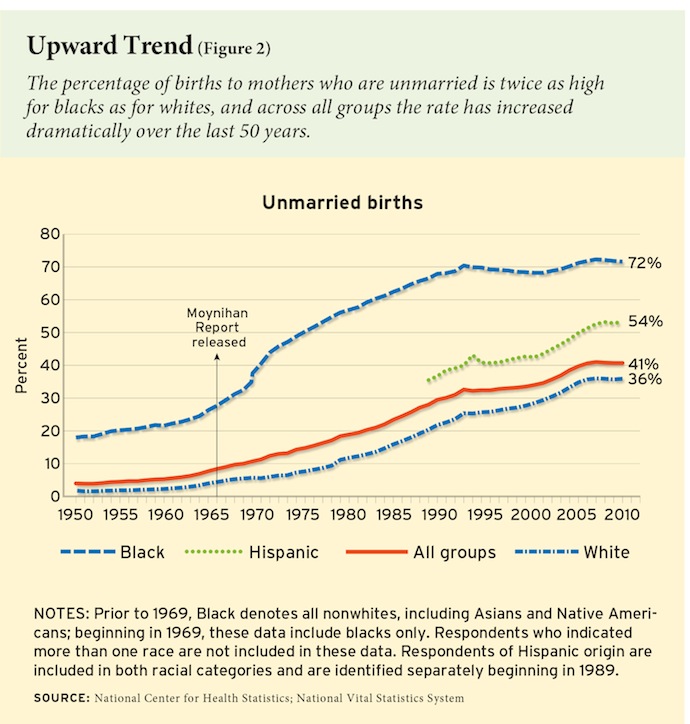
From “Was Moynihan Right?“
But here we are going to concentrate on Whites. In his book Coming Apart Charles Murray notes that for Whites beginning in the 1960s, there has been an increase in crime, lower levels of religiosity, work ethic, and marriage. For the upper-middle class, marriage went from 94% to 84% between 1960 and 2010, but for the White working class it went from 82% to 48%. For the White working class, never-married went from 10% to 25%; and there has been dramatically lower work force participation. Murray attributes this to a loss of “virtue” but he doesn’t discuss the forces and motivation behind this massive cultural shift.
From “Was Moynihan Right?“
It’s common among critics of Murray to claim that these shifts are all about economics rather than the broader culture. From this perspective, in the America of 1963, a high school graduate might expect to find a job which would allow him to marry and permit his wife the leisure to stay home and raise children. He could buy a freestanding house and a car, and still afford to take the family on a two week vacation every summer. The wife would have been reared with a view to preparing her for the duties of marriage and motherhood; she may even have taken ‘Home Ec’ in high school.
The problem with this is that all the trends affecting marriage and the family started in the 1960s when the White working class was doing well, reaching its “heyday” (Case & Deaton) in the early 1970s and stagnating thereafter. The steep upward trend in social/family dysfunction begins in the 1960s and continues to climb until around 1990 when it temporarily falls back before reaching new highs. By 1970, when the White working class was at its economic peak, out of wedlock births had already increased 3-fold from 1960 levels.
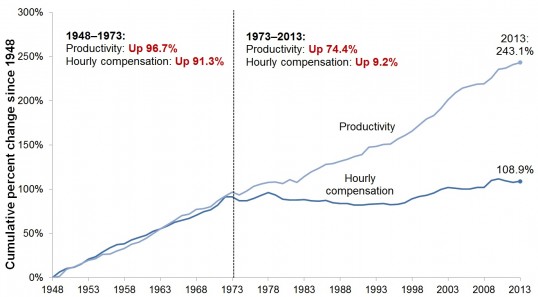
There’s no question that the period from 1948 to the early 1970s was the golden period for the working class (non-supervisory production workers)—strong unions and no outsourcing. But since 1973, the income for this group has actually increased ~9% (Figure 3 of a Pew study[10])—much less than for college-educated, but this is stagnation. It is certainly not a disaster. By itself, it shouldn’t cause increases in mortality given medical advances in the area of heart disease and cancer.
The Opioid Crisis is at the Root of Increased White Mortality
Case and Deaton point out that any economic explanation must explain why stagnant incomes cause early mortality in Whites but not in Blacks or in Europe, and they have a chart showing that “even if we go back to the late 1960s, the ethnic and racial patterns of median family incomes are similar for whites, blacks, and Hispanics, and so can provide no basis for their sharply different mortality outcomes after 1998.” This also rules out widening income inequality (“your income is going up faster than mine”), and it also precludes loss of virtue aided by generous welfare and disability programs because Europeans also have strong programs in these areas.
(However, I should note that recently University of Colorado researchers claim that they will soon be publishing an article showing similar increases in Blacks and Hispanics since 1998,[11] but this still wouldn’t explain why these effects are not seen in Europe in several studies).
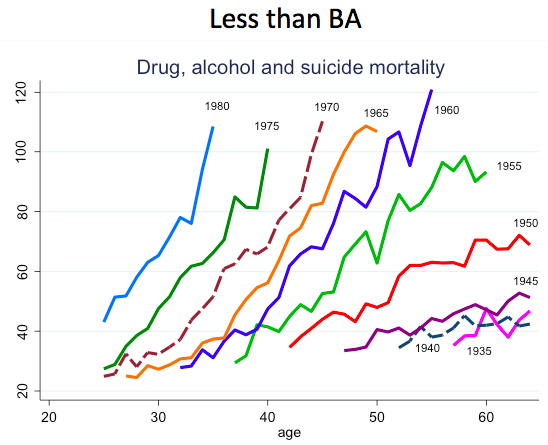
In general, according to Case and Deaton, the increased mortality among the White working class begins in the 1990s. The first cohort to really show increased mortality was the one born in 1950—they were 40 years old in 1990 and thus the first generation to experience the counter-cultural revolution as teenagers. For every cohort after that, the increased mortality from drug poisoning, liver disease, alcohol, and suicide starts at an earlier age and is steeper—it gets to higher levels faster. These trends are higher among men than women and vary by education, with Whites with high school or less showing by far the worst effects.
A 2016 article in the New York Times elaborates on the findings of Case & Deaton based on their examination of 60 million death certificates from 1990–2014, but pins the blame squarely on opioids, not on alcohol or suicide.“[12] “While the death rate among young whites rose for every age group over the five years before 2014, it rose faster by any measure for the less educated, by 23 percent for those without a high school education, compared with only 4 percent for those with a college degree or more.” They also found White mortality much higher than for Black mortality and argued that doctors do not prescribe opiates to Blacks because of fear they may sell them or become addicted, although the previously mentioned study by University of Colorado researchers suggests mortality for Blacks and Hispanics from opioid poisoning is also rising. The Colorado study also agreed with the New York Times study in not finding increases in deaths due to alcoholism and pinned the phenomenon squarely on the opioid epidemic. They note that mortality rates “took off around the time when prescription opioids became readily available, and it has kept rising steadily ever since.”
Given that the trend in mortality may not occur among Blacks and Hispanics and doesn’t occur in Europeans, we can’t suppose that the cultural shifts inaugurated by psychoanalysis are to solely blame. The general decline in the culture is separate from increases in mortality — just because your family relationships are dysfunctional doesn’t mean you are going to die young. However, I suspect that these two factors interact in the sense that if the cultural supports that existed up until the 1950s had remained in place, the White working class would not have succumbed to the opioid epidemic. Again, I stress that people with faster life history profile are less able to control their impulses and thus more prone to maladaptive behavior in a culturally permissive environment awash in drugs and where religious and other cultural constraints on sexuality have been removed. Putting these two things together— the cultural shifts brought about by the triumph of the counter-cultural revolution and the glut of opioid drugs — was a disaster for the White working class. In this regard it’s interesting that the first generation to show increased mortality was the one that became teenagers in the 1960s.
As I have noted, the problems disproportionately affecting the White working class stem from the changes wrought by the 1960s counter-cultural revolution. But the specific problem of increased mortality has to do mainly with opioids, likely in a context where working class Whites are less attached to their jobs—do not find their jobs rewarding, where they have available to them generous disability programs, where they are less likely to gain financially from experience on the job (unlike jobs where promotions are possible), and are more likely to experience pain as a result of their jobs than college-educated Whites. However, the example of European Whites shows that, even with very generous disability payments and the same profile for working class jobs as less rewarding, less likely to benefit from experience, and more likely to result in pain, there has been no upsurge in mortality.
My proposal is that the problem for the White working class is a greedy pharmaceutical industry that has manipulated government regulating agencies and mainstream opinion in the medical profession. A fundamental problem in dealing with this now is the cat is out of the bag. These trends toward increased mortality over 1999 levels will continue no matter what the government does about OxyContin. Increased regulation simply forces addicts into heroin and other illegal drugs. The latest data show that deaths from drug overdoses continue to increase, now around 65,000 per year, despite increased government regulation.
The Sackler Family Is Fundamentally Responsible for the Opioid Crisis.
This all started with Purdue Pharma, owned by the Sackler family. This is an amazing and very depressing story.
Originally, OxyContin-type drugs were used only for severe pain — as continues to be the case in Europe, so their use was quite limited. Purdue’s program was to get OxyContin prescribed for even minor pain. Part of that was to claim that OxyContin was less addictive because it was timed-release, but simply breaking the pill up before swallowing negated the timed-release and they were well aware of that. Their promotional materials emphasized their humanitarian motives—what could be more high-minded than relieving pain without fear of addiction.
Purdue essentially created a very large community of people who benefited financially from prescribing opioids. They set up and funded organizations that lobbied for more aggressive treatment of pain by treatment with opioids. Millions were funneled into organizations like the American Pain Society and the American Academy of Pain Medicine and Purdue’s own advocacy group, Partners Against Pain, as well as to medical professionals willing to provide data supporting the movement. Purdue hired an army of sales reps to promote opioids to all medical personnel, from doctors to physician assistants. A consistent part of the pitch was to minimize addiction rates. Purdue claimed addiction rates were less than 1% by cherry picking studies that did not examine the effects of long-term use.[13] Other studies often showed much higher rates, as high as 50%. This misrepresentation was at the root of the $600M judgement against Purdue obtained by the US government.
The original study claiming very low rates of addiction was in 1986 by R. K. Portenoy based on 38 patients.[14]
Portenoy, of Metropolitan Jewish Health System in New York City, gained renown in the 1980s and 1990s for advocating consideration of opioid painkillers for patients with chronic pain of all kinds, at a time when such use was discouraged. In the 2012 WSJ interview, he conceded that research had not backed up the effectiveness of opioids for these types of pain and that the risks of addiction and other adverse effects were greater than he previously had indicated.
Portenoy also maintains financial relationships with opioid drugmaker Purdue Pharma, as well as other scores of other pharmaceutical companies, many of which have pain offerings: Afferent, Cephalon, CNSBio, Covidien, Endo Pharmaceuticals, Mallinckrodt, Grupo Ferrer, King Pharmaceuticals, NicOx, Prostraken, Shire, Solvay, Wyeth, Xenon, Archimedes, Baxter, Calloway, Flamek, Fralex, GW Pharmaceuticals, and Pfizer.[15]
Once Purdue showed how much money could be made, other pharmaceutical companies jumped into the market. When confronted with data showing that addiction rates were much higher, Portenoy recanted his strong claims but still maintained that opioids were a great treatment for non-cancer pain. And in any case, the damage was already done.
Propublica to their credit has taken a major role in showing how doctors and various organizations benefit from the pharmaceutical industry. It’s a pervasive problem in all areas of medicine,[16] but quite often it’s because they promote drugs that don’t really work compared to placebos. They are not killing tens of thousands of people. Nevertheless, the lesson is to stay away from prescribed drugs as much as possible and do thorough investigations before taking anything. This is an incredibly corrupt industry from top to bottom and it goes way beyond being a specifically Jewish problem. However, the opioid epidemic is in large part a Jewish story.
When it comes to pain management, Propublica emphasizes the roles of two Jewish physicians, Scott Fishman and Perry Fine, prominently associated with the American Pain Foundation which got 88% of its budget from Purdue and other pharmaceutical companies. Fine has been funded by at least a dozen drug companies and Fishman has had relationships with at least eight companies, including Purdue, for which he was a consultant, paid speaker and recipient of research support.[17] They claim that all this financial remuneration did not affect their opinions. And if you believe that, you are an idiot.
The FDA also played an important role, for example, not reviewing Purdue’s promotional literature which included a video that claimed addiction was “very rare”; this was eventually removed, but the damage was done. And of course, even if addiction rates were low when patients used the drug as their doctors intended, many quickly learned to break the tablets up and snort it or inject it. Again, becoming addicted is more likely to occur in people who have less impulse control—those in the lower part of the bell curve.
Purdue left no stone unturned. Hospital accreditation groups also played a role. Hospitals were required by the feds to administer questionnaires to patients recording their pain experience on a 10-point scale, and were threatened with loss of accreditation if they were found to be allowing too much pain.
In 2006, it … became mandatory to poll discharged patients about whether their pain had been adequately assessed and treated during their stay. The change was put in place by the Centers for Medicare and Medicaid Services acting on recommendations of the Joint Commission, the national nonprofit health care quality organization that accredits hospitals [which was funded by Purdue[18]]. The results of these surveys are posted online and they contribute substantially to how the Joint Commission ranks hospitals. The results of these surveys can affect whether or not a hospital is eligible for Medicaid reimbursements, so scoring poorly can affect a hospital’s bottom line. In 2012, the Affordable Care Act made this connection even more direct when it gave Medicare the ability to withhold a portion of hospital reimbursement if patient satisfaction scores were low.
Unsurprisingly, under this regime, the number of opioid prescriptions increased dramatically. Worried that their survey scores would be low for not treating pain aggressively enough (and under pressure to address this), doctors began liberally prescribing opioids.(Jeremy Samuel Faust, ‘The Untold Story of America’s Opioid Addiction’)[19]
Esquire’s Christopher Glazek writes:
Flush with cash, Purdue pioneered a high-cost promotion strategy, effectively providing kickbacks—which were legal under American law—to each part of the distribution chain. Wholesalers got rebates in exchange for keeping OxyContin off prior authorization lists. Pharmacists got refunds on their initial orders. Patients got coupons for thirty-day starter supplies. Academics got grants. Medical journals got millions in advertising. Senators and members of Congress on key committees got donations from Purdue and from members of the Sackler family.
They flew doctors to “seminars’ in fancy vacation destinations. Doctors who didn’t get on board were offered speaking fees to endorse OxyContin.
The feds finally sued Purdue in 2007, with Purdue pleading guilty to felony charges, admitting that it had lied to doctors about OxyContin’s abuse potential. Under the agreement, the company paid $600 million in fines and its three top executives at the time pleaded guilty to misdemeanor charges—after thousands of deaths as a result of their actions. The executives paid $34.5 million out of their own pockets and performed four hundred hours of community service. It was one of the harshest penalties ever imposed on a pharmaceutical company but how can one take it seriously when the people responsible got away with pleading guilty to misdemeanors at a time when by 2001 Purdue was selling $1 billion of OxyContin yearly. In total, Purdue Pharma has made $35 billion, and the Sackler family walked away with around $13 billion.[20]
Misdemeanor pleas for being responsible for the deaths of tens of thousands of people while walking away with billions.
Perhaps the height of cynicism was in 2010, when Purdue reformulated the drug to be less easy to snort—very near the end of its patent on the original version. So it got more years of patent protection.
So the Sackler family is in the clear and is now posing as great humanitarian philanthropists. It’s well known that opioid addiction in mothers has a devastating effect on newborn babies:
Opioid withdrawal, which causes aches, vomiting, and restless anxiety, is a gruesome process to experience as an adult. It’s considerably worse for the twenty thousand or so American babies who emerge each year from opioid-soaked wombs. These infants, suddenly cut off from their supply, cry uncontrollably. Their skin is mottled. They cannot fall asleep. Their bodies are shaken by tremors and, in the worst cases, seizures. Bottles of milk leave them distraught, because they cannot maneuver their lips with enough precision to create suction. Treatment comes in the form of drops of morphine pushed from a syringe into the babies’ mouths. Weaning sometimes takes a week but can last as long as twelve. It’s a heartrending, expensive process, typically carried out in the neonatal ICU, where newborns have limited access to their mothers.[21]
Because of this sort of thing, the Sackler family has been especially motivated to make people think they care about children: “Several have made children a focus of their business and philanthropic endeavors. One Sackler heir helped start an iPhone app called RedRover, which generates ideas for child-friendly activities for urban parents; another runs a child-development center near Central Park; another is a donor to charter-school causes, as well as an investor in an education start-up called AltSchool.
And because they are such wonderful people they have donated to high-profile institutions, always with their name on it. So we have the Sackler Galleries at the Royal Academy Of Arts in London; the Sackler Wing of Oriental Antiquities at the Louvre; The Arthur M. Sackler Gallery at the Smithsonian, Washington, and the Sackler gallery in Ashmolean Museum at Oxford University, The Raymond and Beverly Sackler Institute for Biological, Physical and Engineering Sciences at Yale, and the Sackler School of Graduate Biomedical Sciences at Tufts. There is effusive praise from the beneficiaries. Tufts spokesperson said “It would be impossible to calculate how many lives you have saved, how many scientific fields you have redefined, and how many new physicians, scientists, mathematicians, and engineers are doing important work as a result of your entrepreneurial spirit. You are a world changer.”
So Sackler is being praised for saving lives at a time when the opioid epidemic they started has claimed the lives of over 250,000 mainly White people.
One wonders if the Sacklers would have attempted to engage in such a campaign in Israel. Instead, they established the Sackler Faculty of Medicine, a medical school which is part of Tel Aviv University.
Conclusion
The opioid phenomenon reflects aspects of Jewish activism in general. These are top-down movements that are well-funded, they have access to the most prestigious institutions of the society, and, because of this prestige, they are able to propagate fake science. In the case of the Jewish drive to enact the 1965 immigration law, pro-immigration committees were funded, fraudulent academic studies were created on the benefits of immigration, prominent people were recruited (like JFK, recruited to put his name on a book titled A Nation of Immigrants written by Myer Feldman and published by the ADL), positive articles about immigration appeared in the media, lobbyists and politicians were paid. The main fake scientists discussed in The Culture of Critique were the Boasians with their fake race science (utilized in the debates over the immigration law of 1965), psychoanalysis with its fake sex science, and the Frankfurt School with its fake theory that ethnocentric Whites have a psychiatric disorder resulting from poor parenting. Like the fake scientists who participated in promoting the opioid epidemic, these activists had access to prestigious academic institutions and, in the case of the Frankfurt School and other activist academic research in the 1950s and 1960s, their research was funded by the organized Jewish community, such as the American Jewish Committee, and promoted by Jewish academics.
Or consider the neoconservative infrastructure, with think tanks funded, prominent spokesmen at prestigious universities, and a very large media presence. Neocons can bet that if they are forced out of a job in the Departments of State or Defense that they will have many options to fall back on. Despite promoting disastrous policies, such as the war in Iraq, and despite their obvious ethnic loyalties to Israel, they are still a very powerful component of the U.S. foreign policy establishment.
Jews are an incredibly successful and influential group. We can’t win unless we understand that.
[1] Kevin MacDonald, “Jewish Involvement in Shaping American Immigration Policy, 1881–1965: A Historical Review,” March 1998, accessed December 5, 2017, https://www.researchgate.net/publication/226113583JewishInvolvementinShapingAmericanImmigrationPolicy1881-1965AHistoricalReview.
[2] See, for example, Victor Tan Chen, “All Hollowed Out: The Lonely Poverty of America’s White Working Class, The Atlantic, January 16, 2016, accessed December 5, 2017, https://www.theatlantic.com/business/archive/2016/01/white-working-class-poverty/424341/.
[3] Maya Salam, “The Opioid Epidemic: A Crisis Years in the Making,” the New York Times, October 26, 2017, https://www.nytimes.com/2017/10/26/us/opioid-crisis-public-health-emergency.html?_r=0.
[4] Max Blau, “Opioids Could Kill Nearly 500,000 Americans in the Next Decade,” STAT, June 27, 2017, accessed December 5, 2017, https://www.statnews.com/2017/06/27/opioid-deaths-forecast/.
[5] Anne Case & Angus Deaton, ‘Mortality and morbidity in the 21st century,’ https://www.brookings.edu/wp-content/uploads/2017/03/6_casedeaton.pdf
[6] ‘The psychometric assessment of human life history strategy: A meta-analytic construct validation,’ accessed December 5, 2017: https://www.researchgate.net/publication/262972058_The_psychometric_assessment_of_human_life_history_strategy_A_meta-analytic_construct_validation
[7] Roger Clegg, ‘Latest Statistics on Out-of-Wedlock Births,’ National Review, Oct 11 2013, http://www.nationalreview.com/corner/360990 accessed December 5, 2017.
[8] M.P. Dunne, ‘Genetic and Environmental Contributions to Variance in Age at First Sexual Intercourse,’ http://journals.sagepub.com/doi/abs/10.1111/j.1467-9280.1997.tb00414.x, accessed December 5, 2017.
[9] G.A. Akerlof, ‘An Analysis of Out-Of-Wedlock Births in the United States,’ August 1996, https://www.brookings.edu/research/an-analysis-of-out-of-wedlock-births-in-the-united-states/, accessed December 5, 2017.
[10] Lawrence Michel, Elise Gould & Joel Bivens, ‘Wage Stagnation in Nine Charts,’ Economic Policy Institute, January 6, 2015, www.epi.org/publication/charting-wage-stagnation/, accessed December 5, 2017.
[11] ‘Opioids and obesity, not ‘despair deaths,’ raising mortality rates for white Americans,’ Science Daily, July 20, 2017, https://www.sciencedaily.com/releases/2017/07/170720142334.htm, accessed December 5, 2017.
[12] Gina Kolata & Sarah Cohen, ‘Drug Overdoses Propel Rise in Mortality Rates of Young Whites,’ New York Times, January 16, 2016, https://www.nytimes.com/2016/01/17/science/drug-overdoses-propel-rise-in-mortality-rates-of-young-whites.html?_r=0, accessed December 5, 2017.
[13] Art Van Zee, ‘The Promotion and Marketing of OxyContin: Commercial Triumph, Public Health Tragedy,’ American Journal of Public Health, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2622774/, accessed December 5, 2017.
[14] R.K. Portenoy and K.M. Foley, ‘Chronic use of opioid analgesics in non-malignant pain: report of 38 cases,’ May 1986, https://www.ncbi.nlm.nih.gov/pubmed/2873550, accessed December 6, 2017.
[15] Portenoy Opioid Talk Sparks Controversy: Opioid advocate Russell Portenoy’s invitation to an upcoming NIH workshop is under fire. Medpage Today, https://www.medpagetoday.com/painmanagement/painmanagement/47855, accessed December 22, 2017.
[16] See for example, Alison Bass, Side Effects: A Prosecutor, a Whistleblower, and a Bestselling Antidepressant on Trial (Algonquin Books of Chapel Hill, 2008); Melody Petersen, Our Daily Meds: How the Pharmaceutical Companies Transformed Themselves into Slick Marketing Machines and Hooked the Nation on Prescription Drugs (Farrar, Straus and Giroux, 2008); Christopher Lane, Shyness: How Normal Behavior Became a Sickness (Yale University Press, 2008).
[17] https://www.documentcloud.org/documents/279187-responsible-opioid-prescribing-info, accessed December 7, 2017.
[18] Report to Congressional Requesters, ‘Prescription Drugs,’ December 2003, https://www.gao.gov/new.items/d04110.pdf, accessed December 7, 2016.
[19] Jeremy Samuel Faust, ‘The Untold Story of America’s Opioid Addiction,’ Slate, June 3, 2016, http://www.slate.com/articles/health_and_science/medical_examiner/2016/06/prince_s_death_reveals_how_wrong_our_over_reliance_on_dangerous_opioids.html, accessed, December 7, 2017.
[20] Vijay Prashad, ‘Big Pharma’s Pushers: the Corporate Roots of the Opioid Crisis,’ Counterpunch, November 17, 2017, https://www.counterpunch.org/2017/11/10/big-pharmas-pushers-the-roots-of-the-opioid-crisis/, accessed December 7, 2017.
[21] Christopher Glazek, ’The Secretive Family Making Millions from the Opioid Crisis,’ Esquire, October 16, 2017, http://www.esquire.com/news-politics/a12775932/sackler-family-oxycontin/, accessed December 7, 2017.



Comments are closed.